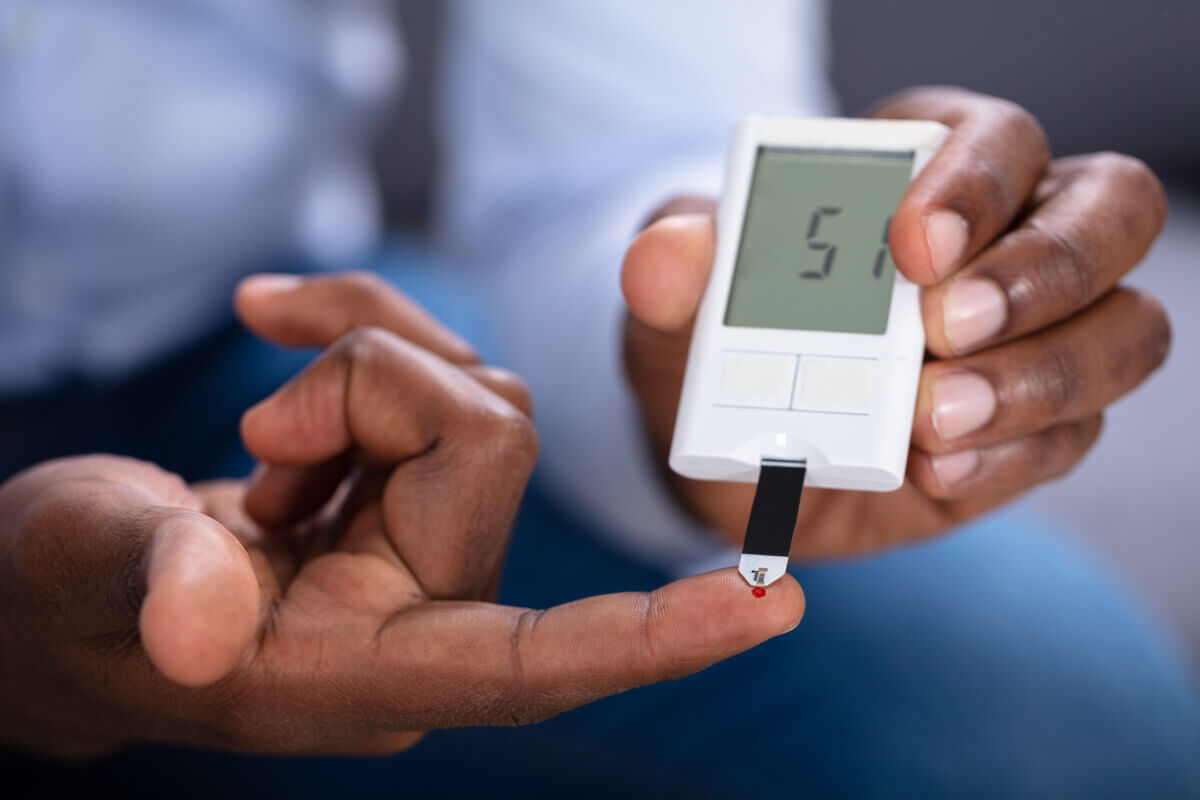
Cutting carbs shows promise in naturally boosting insulin production for people with Type 2 diabetes. (Chinnapong/Shutterstock)
In a nutshell
- A very low-carb diet (just 9% of daily calories from carbs) significantly improved the pancreas’s ability to produce insulin in people with mild Type 2 diabetes, within just 12 weeks.
- These improvements happened without weight loss and were stronger than what current diabetes medications typically achieve.
- Different racial groups responded in different ways: African American participants showed a bigger boost in early insulin response, while European Americans had greater improvements in overall insulin output.
BIRMINGHAM, Ala. — Drug companies are racing to treat Type 2 diabetes, but your own body might already hold the key to better blood sugar control. In a new study from the University of Alabama, people with diabetes who slashed carbs to just 9% of their daily diet saw a major boost in their pancreas’s ability to produce insulin, within just three months. That kind of turnaround hasn’t been seen with any medication currently on the market.
First-phase insulin secretion, the first wave of insulin your pancreas releases right after you eat or when your blood sugar rises, plays a vital role in efficiently clearing glucose from the bloodstream after meals. In fact, despite medication, pancreatic function usually continues to decline as Type 2 diabetes progresses.
The research, published in The Journal of Clinical Endocrinology & Metabolism, showed that a low-carb diet may actually fix the root problem in the pancreas, instead of just covering up the symptoms.
The study compared two groups of patients with Type 2 diabetes. One group followed a carbohydrate-restricted diet, deriving only about 9% of energy from carbohydrates and 65% from fat, while the control group ate a higher-carbohydrate diet with approximately 55% of energy from carbohydrates and 20% from fat. Both diets contained the same amount of protein (about 25-26%) and were designed to maintain body weight rather than promote weight loss.

After 12 weeks, those on the low-carb diet showed double the first-phase insulin response compared to the higher-carb group. The researchers also saw improvements in the pancreas’s overall ability to make and respond to insulin. Longer treatment periods or additional weight loss might yield even more significant improvements in pancreatic function.
This could be a potential path to diabetes remission that doesn’t require invasive bariatric surgery or extremely restrictive very-low-calorie diets, which are currently the only interventions known to potentially reverse the disease.
The study enrolled 57 African American and European American adults with mild Type 2 diabetes (diagnosed within the past 10 years and with HbA1c levels below 8.0). All participants had to stop taking their diabetes medications 1-2 weeks before baseline testing and throughout the 12-week trial. While three participants had to resume taking metformin during the study, the others maintained stable blood glucose levels without medication.
While both African Americans and European Americans showed improvements, they responded differently to the low-carb diet. African Americans had greater improvements in acute insulin response (the first-phase response), increasing by 110%, while European Americans showed greater improvements in maximal insulin response, the pancreas’s full capacity to release insulin, increasing by 48%.
Previous studies have shown that African Americans typically have a higher insulin response to glucose than European Americans, even when matched for insulin sensitivity. This heightened responsiveness could potentially lead to more pancreatic stress over time.
In another 48-week study mentioned by the authors, low-carb diets had favorable effects on blood pressure and HbA1c levels compared to low-fat diets, despite identical weight loss between groups. By the end of that study, 70% of patients on the low-carb diet had reduced their medication use by at least half.
This research shows promising results, but dramatically cutting carbohydrates may be challenging for some patients. The low-carb diet in this study allowed only about 9% of calories from carbohydrates, far lower than the typical American diet, which derives roughly 50% of calories from carbs.
Nevertheless, these findings suggest that carbohydrate restriction could offer a viable first-line approach for managing Type 2 diabetes. Unlike medications, which merely treat symptoms while the disease progresses, changing your diet appears to tackle issues in your pancreas.
For the millions of Americans living with Type 2 diabetes, these results offer hope that simple dietary changes could potentially slow or even reverse disease progression, reducing reliance on medications and lowering the risk of complications. By improving pancreatic function at the cellular level, carbohydrate restriction may finally provide a path to addressing the root cause of the disease rather than just managing its symptoms.
Paper Summary
Methodology
The researchers conducted a 12-week randomized clinical trial involving 57 African American and European American adults diagnosed with Type 2 diabetes within the past 10 years. Participants had BMIs between 25-50 and HbA1c levels below 8.0, and were not using insulin therapy. All participants discontinued their diabetes medications 1-2 weeks prior to baseline testing. They were randomly assigned to either a carbohydrate-restricted (CR) diet (approximately 9% energy from carbohydrates, 26% from protein, and 65% from fat) or a higher-carbohydrate (HC) diet (approximately 55% energy from carbohydrates, 25% from protein, and 20% from fat). Both diets were designed to be weight-maintaining, with calories adjusted weekly if weight changed by more than 1 kg. Participants received detailed meal plans and groceries were delivered weekly, though they prepared their own meals. The researchers assessed β-cell function using a hyperglycemic clamp to measure both acute (first-phase) and maximal (arginine-stimulated) C-peptide responses to glucose at baseline and after 12 weeks. They also conducted a 3-hour oral glucose tolerance test to calculate the disposition index, which reflects overall β-cell function.
Results
After 12 weeks, participants on the carbohydrate-restricted diet showed significantly improved β-cell function compared to those on the higher-carbohydrate diet. The acute C-peptide response was two-fold greater in the CR group (p < 0.01) across all participants, with a particularly strong effect in African Americans (110% greater, p < 0.01). The maximal C-peptide response was 22% greater in the CR group (p < 0.05) overall, with European Americans showing the strongest improvement (48% greater, p < 0.01). The disposition index, which measures overall β-cell function, was 32% greater in the CR group (p < 0.05) after 12 weeks, with the effect most pronounced in African Americans (48% greater, p < 0.01). Importantly, insulin sensitivity did not change significantly with either diet intervention, suggesting that the improvements came directly from enhanced β-cell function rather than reduced insulin resistance. The CR diet also led to higher β-hydroxybutyrate levels, indicating nutritional ketosis.
Limitations
The study had several limitations. The sample size was relatively small, with only 57 participants completing the trial out of 65 enrolled. The intervention lasted only 12 weeks, so long-term effects remain unknown. The study focused on patients with mild Type 2 diabetes (HbA1c < 8.0), so results may not generalize to those with more severe disease. The researchers noted that while all food was provided, participants prepared their own meals, potentially introducing variability in adherence. Additionally, the dramatic carbohydrate restriction (to just 9% of calories) might be difficult for many patients to maintain in real-world settings. The study also relied on self-reported race, which is an imperfect proxy for biological differences.
Funding/Disclosures
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (R01DK116726), the UAB Nutrition Obesity Research Center (P30DK56336), and the UAB Diabetes Research Center (P30DK079626). One of the authors was supported by the National Heart, Lung, and Blood Institute (T32HL105349). The authors declared no conflicts of interest.
Publication Information
The paper titled “Effects of a Carbohydrate-Restricted Diet on β-Cell Response in Adults With Type 2 Diabetes” was published in The Journal of Clinical Endocrinology & Metabolism in October 2024. The lead authors were Barbara A. Gower, Amy M. Goss, Marian L. Yurchishin, Sarah E. Deemer, Bhuvana Sunil, and William T. Garvey from the Department of Nutrition Sciences at The University of Alabama at Birmingham and the Division of Pediatric Endocrinology at Children’s of Alabama.